Bridging Medical Model and Social Model of Disability Awareness 2026-27🎯
What distinguishes medical models and social models of disability? 🎯
Understand how bridging Medical Model and Social Model of disability shapes inclusive education and policy for better student outcomes in 2026-27.

Disclaimer: This article is provided for educational and informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified professional with any questions you may have regarding a medical condition or educational needs. Visit full page disclaimer https://dp-ho.com/disclaimer-page/.
ڈس کلیمر: یہ مضمون صرف تعلیمی اور معلوماتی مقاصد کے لیے فراہم کیا گیا ہے۔ اس کا مقصد کسی بھی قسم کا پیشہ ورانہ طبی مشورہ، تشخیص یا علاج فراہم کرنا نہیں ہے۔ طبی حالت یا تعلیمی ضروریات سے متعلق اپنے کسی بھی سوال کے لیے ہمیشہ کسی مستند ماہر سے مشورہ کریں۔ مزید تفصیل کے لیئے ڈسکلیمر پیج کو دیکھیں
https://dp-ho.com/disclaimer-page/
مختصر خلاصہ (Brief Summary)
طبی ماڈل (Medical Model): اس کا بنیادی فوکس فرد کی تشخیص، علاج اور اس کی جسمانی یا ذہنی کمی کو “ٹھیک” کرنے پر ہوتا ہے۔ اس میں معذوری کو ایک طبی مسئلہ سمجھا جاتا ہے جسے ماہرین کی مدد سے حل کرنا مقصود ہوتا ہے۔
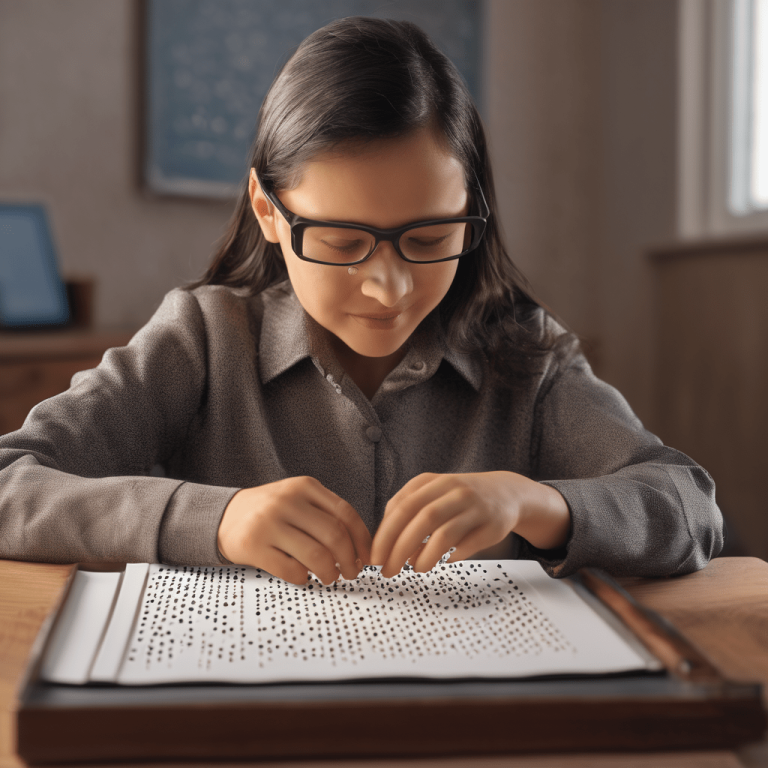
سماجی ماڈل (Social Model): یہ ماڈل کہتا ہے کہ اصل مسئلہ فرد کی جسمانی حالت نہیں، بلکہ معاشرے کا رویہ، انفراسٹرکچر اور نظامی رکاوٹیں ہیں (مثلاً اگر کسی اسکول میں ریمپ نہیں ہے تو بچہ خود معذور نہیں، بلکہ عمارت کا ڈھانچہ اس کے لیے رکاوٹ ہے)۔
ان دونوں کا امتزاج (The Bridge): ایک ماہرِ تعلیم کی حیثیت سے، میرا ماننا ہے کہ ہمیں ان دونوں کو ملانے کی ضرورت ہے۔ ہمیں طلباء کی طبی ضروریات (Therapy/Clinical Support) کو نظر انداز نہیں کرنا چاہیے، لیکن ساتھ ہی ساتھ تعلیمی ماحول (Environment) کو اتنا جامع (Inclusive) بنانا چاہیے کہ کوئی بھی طالب علم خود کو معاشرتی رکاوٹوں کی وجہ سے پیچھے نہ سمجھے۔
خلاصہ یہ کہ: جب ہم طبی سہولیات کو سماجی شمولیت کے ساتھ جوڑتے ہیں، تب ہی ہم 2026-27 کے جدید معیارات کے مطابق ایک ایسا تعلیمی نظام بنا سکتے ہیں جہاں ہر طالب علم اپنی پوری صلاحیت کے ساتھ کامیابی حاصل کر سکے۔
Reconciling Medical Model and Social Model Paradigms in Special Education 🎯
The Medical Model and Social Model represent the two pillars of disability theory. Understanding the tension—and the potential for harmony—between these frameworks is essential for any special education expert aiming to provide truly equitable support in the 2026-27 landscape.
The Medical Model: Pathology and Clinical Intervention 🎯
The medical model defines disability through the narrow lens of pathology. It views an individual’s condition as a deviation from the “norm” that requires diagnosis and clinical intervention. Under this paradigm:
- Focus on Diagnosis: The primary goal is to identify a “deficit” or biological impairment that necessitates treatment, medication, or specialized therapy.
- The Individual as Patient: The student is often viewed as someone who needs to be “fixed” or “cured” to better fit into the existing structure of society.
- Burden of Change: In this view, the burden of change lies entirely on the individual. The student is expected to adapt to the environment through clinical progress.
The Social Model: Dismantling Systemic Barriers 🎯
In sharp contrast, the social model of disability posits that individuals are not disabled by their conditions, but by systemic barriers. It argues that society is constructed for the “average” human, and those who fall outside that construction face exclusion.
- Environment as the Barrier: A student in a wheelchair is not disabled by their inability to walk, but by the absence of ramps.
- Reframing Disability: Disability is seen as a social construct created by negative attitudes, inaccessible infrastructure, and rigid pedagogical structures.
- The Burden of Change: Under this model, the burden of change shifts from the student to society. It is the school’s responsibility to modify the environment to ensure full inclusion.
Bridging the Medical Model and Social Model 🎯
Bridging the Medical Model and Social Model is essential for a comprehensive educational strategy. If we only utilize the medical model, we risk pathologizing students and ignoring their need for a barrier-free world. If we rely solely on the social model, we may fail to provide the necessary clinical support, such as speech therapy or sensory aids, that can drastically improve a student’s quality of life.
Creating a Supportive Ecosystem
By acknowledging the clinical need for therapy while simultaneously dismantling environmental hurdles, we create a supportive ecosystem that treats the student as a whole person. This hybrid approach ensures:
- Clinical Support: Students receive the medical/therapeutic interventions they need to thrive physiologically.
- Environmental Access: The school infrastructure, teaching materials, and social atmosphere are adjusted to meet the student’s unique needs, not the other way around.
- Holistic Autonomy: The student gains both the functional skills (from medical support) and the societal access (from social support) required for true independence.
Reconciling the Medical Model and Social Model creates a powerful synergy. It allows us to advocate for systemic change while providing the individualized clinical care that IDEA and other procedural safeguards demand. This integrated perspective is the cornerstone of effective, modern special education.
Reconciling Medical Model and Social Model Paradigms in Special Education 🎯
The Medical Model and Social Model represent the two foundational pillars of disability theory. Understanding the tension and the potential for harmony between these frameworks is essential for any special education expert aiming to provide truly equitable support in the 2026-27 landscape. As educators, we must navigate how these perspectives shape IEP goals, classroom design, and the overall lived experience of our students.
The Medical Model, Pathology and Clinical Intervention 🎯

The medical model defines disability through the narrow lens of pathology and deficit. It views an individual’s condition as a deviation from the “norm” that requires diagnosis and clinical intervention by specialized professionals. Under this paradigm:
- Focus on Diagnosis: The primary goal is to identify a “deficit” or biological impairment that necessitates treatment, medication, or specialized clinical therapy.
- The Individual as Patient: The student is often viewed as a patient who needs to be “fixed” or “cured” to better fit into the existing structure of society.
- Burden of Change: In this view, the burden of change lies entirely on the individual. The student is expected to adapt to the environment through clinical progress and therapeutic intervention.
The Social Model: Dismantling Systemic Barriers 🎯
In sharp contrast, the Medical Model and Social Model perspective highlights that the social model of disability posits that individuals are not disabled by their conditions, but by systemic barriers. While the Medical Model and Social Model dialogue often centers on clinical diagnosis, the social model argues that society is constructed for the “average” human, and those who fall outside that construction face exclusion.
Environment as the Primary Barrier 🎯
The distinction between the Medical Model and Social Model is best seen in physical access. A student in a wheelchair is not disabled by their inability to walk, but by the absence of ramps. Similarly, a deaf student is not disabled by their hearing loss, but by a lack of access to sign language or visual communication tools. When we fail to bridge the Medical Model and Social Model, we inadvertently blame the student for failing to navigate a world that was never designed for them.
Reframing Disability as a Social Construct 🎯
Disability is re-envisioned through the Medical Model and Social Model lens as a social construct created by negative attitudes, inaccessible infrastructure, and rigid pedagogical structures. These structures often fail to account for neurodiversity. If we strictly follow only one side of the Medical Model and Social Model framework, we miss the opportunity to foster true belonging. Reframing disability means looking at the environment—not the individual—as the primary locus of change.
The Burden of Change in Education 🎯
Under this inclusive framework, the burden of change shifts from the student to society. It is the school’s and the educator’s responsibility to modify the environment to ensure full inclusion, rather than expecting the student to “perform” normality. By actively reconciling the Medical Model and Social Model, educators can identify and dismantle these hidden barriers. This shift is vital for any comprehensive strategy, as a balanced approach ensures that we support the individual’s biological needs while simultaneously removing the societal hurdles that impede their success. Balancing the Medical Model and Social Model is the ultimate goal of modern, inclusive pedagogy.
Bridging the Medical Model and Social Model 🎯
Bridging the Medical Model and Social Model is essential for a comprehensive educational strategy. If we only utilize the medical model, we risk pathologizing students and ignoring their need for a barrier-free world. If we rely solely on the social model, we may fail to provide the necessary clinical support—such as speech therapy, occupational therapy, or sensory aids—that can drastically improve a student’s physiological quality of life.
Creating a Supportive Ecosystem 🎯
By acknowledging the clinical need for therapy while simultaneously dismantling environmental hurdles, we create a supportive ecosystem that treats the student as a whole person. This hybrid approach ensures:
- Clinical Support: Students receive the medical or therapeutic interventions they need to thrive physiologically. This recognizes the biological reality of the student’s condition without labeling the person as “broken.”
- Environmental Access: The school infrastructure, teaching materials, and social atmosphere are adjusted to meet the student’s unique needs. This honors the student’s right to participate fully in the learning community.
- Holistic Autonomy: The student gains both the functional skills (provided by medical/therapeutic support) and the societal access (provided by social support) required for true independence and agency.
The Synergistic Future of Special Education 🎯
Reconciling the Medical Model and Social Model creates a powerful synergy. It allows us to advocate for broad, systemic change while providing the individualized, precision-based clinical care that IDEA and other procedural safeguards demand.
In 2026-27, an expert educator does not choose one model over the other. Instead, they operate at the intersection of both. This integrated perspective is the cornerstone of effective, modern special education, ensuring that every student is not just “accommodated,” but genuinely empowered to succeed.
Reconciling Medical Model and Social Model Paradigms in Special Education 🎯

The Medical Model and Social Model represent the two foundational pillars of disability theory. Understanding the tension and the potential for harmony between these frameworks is essential for any special education expert aiming to provide truly equitable support in the 2026-27 landscape. As educators, we must navigate how these perspectives shape IEP goals, classroom design, and the overall lived experience of our students.
The Medical Model: Pathology and Clinical Intervention 🎯
The medical model defines disability through the narrow lens of pathology and deficit. It views an individual’s condition as a deviation from the “norm” that requires diagnosis and clinical intervention by specialized professionals. Under this paradigm, education is often secondary to correction.
Core Components of the Medical Model:
- Focus on Diagnosis: The primary goal is to identify a “deficit” or biological impairment that necessitates treatment, medication, or specialized clinical therapy. It seeks to categorize the child according to a clinical label to unlock services.
- The Individual as Patient: The student is often viewed as a patient who needs to be “fixed” or “cured” to better fit into the existing structure of society. The focus remains on what the student cannot do.
- Burden of Change: In this view, the burden of change lies entirely on the individual. The student is expected to adapt to the environment through clinical progress, medication, or therapeutic intervention to reach “typical” developmental milestones.
The Social Model: Dismantling Systemic Barriers 🎯
In sharp contrast, the social model of disability posits that individuals are not disabled by their conditions, but by systemic barriers. It argues that society is constructed for the “average” human, and those who fall outside that construction face exclusion.
Core Components of the Social Model:
- Environment as the Barrier: A student in a wheelchair is not disabled by their inability to walk, but by the absence of ramps and elevators. Similarly, a deaf student is not disabled by their hearing loss, but by a lack of access to sign language, captioning, or visual communication tools.
- Reframing Disability: Disability is re-envisioned as a social construct created by negative attitudes, inaccessible infrastructure, and rigid pedagogical structures that fail to account for neurodiversity and physical diversity.
- The Burden of Change: Under this model, the burden of change shifts from the student to society. It is the school’s and the educator’s responsibility to modify the environment to ensure full inclusion, rather than expecting the student to “perform” normality.
Bridging the Medical Model and Social Model 🎯
Bridging the Medical Model and Social Model is essential for a comprehensive educational strategy in 2026-27. If we only utilize the medical model, we risk pathologizing students and ignoring their need for a barrier-free world. If we rely solely on the social model, we may fail to provide the necessary clinical support—such as speech therapy, occupational therapy, or sensory aids—that can drastically improve a student’s physiological quality of life.
Creating a Supportive Ecosystem 🎯
By acknowledging the clinical need for therapy while simultaneously dismantling environmental hurdles, we create a supportive ecosystem that treats the student as a whole person. This hybrid approach ensures:
- Clinical Support: Students receive the medical or therapeutic interventions they need to thrive physiologically. This recognizes the biological reality of the student’s condition without labeling the person as “broken.”
- Environmental Access: The school infrastructure, teaching materials, and social atmosphere are adjusted to meet the student’s unique needs. This honors the student’s right to participate fully in the learning community.
- Holistic Autonomy: The student gains both the functional skills (provided by medical/therapeutic support) and the societal access (provided by social support) required for true independence and agency in their transition to adulthood.
The Synergistic Future of Special Education 🎯
Reconciling the Medical Model and Social Model creates a powerful synergy. It allows us to advocate for broad, systemic change while providing the individualized, precision-based clinical care that IDEA and other procedural safeguards demand.
In 2026-27, an expert educator does not choose one model over the other. Instead, they operate at the intersection of both. This integrated perspective is the cornerstone of effective, modern special education, ensuring that every student is not just “accommodated,” but genuinely empowered to succeed. This balanced approach is the future of truly inclusive, equitable education.
Which strategies support parents and educators through a hybrid framework? 🎯
Effective transition planning requires a sophisticated hybrid approach that refuses to choose between clinical support and environmental access. When parents formally request Transition Services, they are essentially demanding that the school district acknowledge both the biological realities addressed by the Medical Model and Social Model of environmental access. By moving beyond a narrow clinical scope, educators can create a comprehensive roadmap for student independence.
Implementing the Hybrid Strategy in IEP Meetings 🎯
To successfully navigate the integration of the Medical Model and Social Model, parents and educators should utilize a collaborative planning matrix. This ensures that the IEP team does not view clinical therapy and environmental modification as competing interests, but as complementary tools for success.
| Feature | Medical Model and Social Model Integration Matrix |
| Primary Goal | Transitioning from remediation to life-long holistic success |
| Authority | Clinical experts and self-advocates working as a collaborative team |
| Primary Tools | Balancing therapy with assistive AI and structural modifications |
| Student Focus | Treating the student as a whole person, not just a set of deficits |
By adopting this balanced framework, we empower parents to advocate for their child’s dignity rather than just focusing on “fixing” a condition. My work at Special Ed Authority specifically focuses on facilitating this transition, helping families view the student as a person first—a core tenet when bridging the Medical Model and Social Model.
How have success stories shaped our inclusive policy? 🎯
The most powerful evidence for bridging the Medical Model and Social Model comes from real-world success stories. I recall a student with profound hearing loss whose initial clinical diagnosis suggested only high-cost, invasive hardware to “correct” his hearing. By shifting our perspective to balance the Medical Model and Social Model, we stopped focusing solely on the hardware and began modifying classroom acoustics and social interaction norms.
The student thrived because we moved away from the attempt to “fix” the hearing loss and transitioned toward accommodating the learner. This shift transformed his academic experience from one of constant struggle to one of participation. You can read more about similar interventions and my specialized field experience at Special Ed Authority and my research portal.
Why must we prioritize the person over the diagnosis? 🎯
When educators and parents ignore the synergy between the Medical Model and Social Model, students often experience “educational fatigue,” where the sheer volume of clinical intervention overshadows their social development. By prioritizing the person, we ensure that the Medical Model and Social Model serve the student’s long-term goals.
Whether it is through Transition Services or daily classroom adjustments, the hybrid approach remains the gold standard for 2026-27. This perspective not only improves academic outcomes but also builds a foundation for advocacy, allowing the student to navigate a world that is gradually becoming more accessible due to the reconciliation of the Medical Model and Social Model.ons at dp-ho.com.
10 Frequently Asked Questions (FAQs) 🎯
- How do the Medical Model and Social Model differ? The medical model prioritizes clinical diagnosis, while the social model prioritizes environmental and societal change.
- Can these models coexist? Absolutely; a hybrid approach treats the medical need while removing societal barriers.
- What is the role of the IEP in this framework? The IEP acts as the legal bridge that turns medical data into actionable social accommodations.
- How does AI improve inclusion? AI creates adaptable learning environments that reduce the need for individual “remediation.”
- Where can I find more on disability legislation? Visit IDEA resources for federal compliance standards.
- Are parents legally entitled to this hybrid approach? Yes, Procedural Safeguards guarantee that parental input shapes all accommodation decisions.
- Does the social model ignore medical needs? No; it argues that the medical need should not define the person’s value.
- How do I explain these models to school staff? Focus on how both perspectives lead to better student participation.
- Is research available on this topic? Yes, Google Scholar contains extensive literature.
- Where can I learn more about your research? Visit dp-ho.com for my expert articles on hearing impairment.
Key Takeaways for Sharing
“Bridging the Medical Model and Social Model is not just theory; it is the path to true empowerment and long-term student success.” — Imtiyaz Ali
References:
- Shakespeare, T. (2025). Disability Rights and Social Theory.
- U.S. Dept of Education. (2026). IDEA Annual Report to Congress.
- WHO. (2025). Global Report on Equity in Health.
Disclaimer: This article is for information only. Please read our full Disclaimer.
Urdu version
ڈس کلیمر: یہ مضمون صرف معلومات کے لیے ہے۔ براہ کرم ہمارا مکمل ڈس کلیمرپڑھیں۔